The year 2020 has presented tremendous challenges and changes to all fields of medicine. As this pandemic has grown in size and impact, there has been growing concern about the impact of social, economic and political stressors on mental health (MH). Early data from the CDC has shown rising prevalence of symptoms of anxiety, substance abuse, suicidal ideations, and depressive disorders across all ages, with a disproportionate prevalence amongst young adults (62.9% in 18-24yo vs 30.9% in all ages) and racial minorities.1 Data on children and teens is still being collected, but thus far points to similar increases in children and teens.2 As COVID continues to affect our communities, physicians must be on alert for these growing psychiatric concerns.
One of the major changes for youth has been the closure of schools and subsequent shift to online education. Children of all ages across the state are now learning virtually and screen time is surpassing the limits recommended by AAP. While public opinion often considers social media as having a negative impact on MH, the data around this is mixed.4,5 Rather than focusing on social media use itself, it may be more helpful to look at specific exposures to negative aspects of social media, such as online bullying, sexual exploitation, and trauma exposure.5,6 An example that has received considerable media attention this year is the prevalence across social media platforms of videos depicting police brutality of minorities. The American Academy of Child and Adolescent Psychiatry (AACAP) recommends parents have an active, hands on role in helping children process information they have learned from the news about tragedies.3 When children view these images on social media, they often lack the parental support and context, and may experience higher stress related responses.7 As screen time increases, parents should be advised to remain engaged in what their children are viewing and how they are processing that information. Physicians should also be ready to discuss in detail how patients are using their screen time and how it may be affecting their mood and thoughts.
Cannabis, also known as Marijuana, remains the most used illegal drug in the United States. National estimates suggest that 22.2 million people 12 years or older are current users of Cannabis. The primary cannabinoids in cannabis are 9-Tetrahydrocannabinol (THC) and cannabinol (CBD). THC is primarily responsible for the psychoactive properties of cannabis. Cannabinoids are thought to exert their pharmacological activity via several mechanisms. The most studied is the receptor mediated mechanism that includes two receptors, Cannabinoid-binding receptor 1 (CB1) and Cannabinoid-binding receptor 2 (CB2). CB1 receptors are located throughout the central nervous system (CNS) and CB2 are only found in the peripheral tissues. Stimulation of the receptors in the CNS produces hallucinations, memory loss, dyskinesia, and sedation. The actions of CB2 are receptors are not yet clear.
The increase in legalization, availability, and marketing of cannabis, correlates to an increase in unintentional pediatric exposures. Pediatric exposures to cannabis rose from 148% from 2006 to 2013. Since the decriminalization of cannabis, there has been an explosion of dispensaries that have catapulted cannabis to be a major industry generating $ 2.3 billion dollars in sales in Colorado alone. Part of this growth has included expansion in the available forms of cannabis, including edible products, concentrated tinctures, and e-cigarettes. Many commercial cannabis-infused edibles are produced in the form of cookies, cakes, candy bars, and even drinks, which are indistinguishable to children from their non-cannabis counterparts. Edibles have become the most common form of unintentional cannabis exposure in pediatrics.
The Center for Disease Control and Prevention (CDC) defines sudden unexpected infant death (SUID) as “the sudden death of an infant under 1 year of age that cannot be explained after a thorough investigation.” SUID is routinely classified as: 1) sudden infant death syndrome (SIDS), 2) accidental suffocation and strangulation in bed (ASSB), or 3) death from unknown causes. Each year, around 4,000 U.S. babies die from SUID, making it an important topic to understand and effect change. In Georgia, there are three deaths every week from SUID. Between 1990 and 1999, the SUID rate drastically declined following numerous safe sleep campaigns, the most notable being the “Back to Sleep” campaign in 1994. In 2012, the AAP expanded their focus to include environmental recommendations (such as sleep location and environment) and renamed it the “Safe to Sleep” campaign. Since 1997, SIDS deaths have become less common; however, rates of infant death due to unknown causes and ASSB are stagnant. With proper safe sleep education and adherence to the American Academy of Pediatrics (AAP) safe sleep recommendations, the risk of sleep-related infant death can be reduced.
A 12-year-old boy presented to the emergency department with 3 days of fever, vomiting for one day and rash. On presentation he was febrile to 38.5 C, tachycardic to 122, and had normal blood pressure, oxygen saturations and respiration rate. His exam was notable for a sandpaper rash and mild conjunctivitis. He later tested positive for SARS-CoV-2 antibodies. This is an example of a patient who was determined to have Multisystem Inflammatory Syndrome in Children (MIS-C), understood to be a post-viral inflammatory response to SARS-CoV-2. This article will briefly review SARS-CoV-2 infections in children, the MIS-C phenomenon, and recommendations for transfer.
While the majority of children exhibit mild symptoms when infected with SARS-CoV-2, a unique picture of how the virus impacts children continues to evolve. Early epidemiological studies from China and Italy showed that up to one-fifth of infected children were asymptomatic, half were mild and had only upper respiratory symptoms, about a third had pneumonia but without respiratory distress or hypoxemia, and 1% had severe infections.
In late March, physicians in Italy and the United Kingdom noticed higher numbers children presented to their hospitals with some stigmata of Kawasaki disease. Some became very ill with vasodilatory shock and some showed signs of severe inflammatory reactions consistent with macrophage activation syndrome. Many exhibited cardiovascular compromise and needed various forms of support: intubation, inotropes, and even extracorporeal membrane oxygenation. They tended to be lymphopenic and thrombocytopenic, with high inflammatory markers like CRP, ESR, ferritin, d-dimer, and cardiac markers if the disease progressed to the cardiovascular system. They tended to be older than traditional Kawasaki disease pateints.4,5
Soon after, similar cases were noticed in the United States, initially in New York. To better define this phenomenon, it was given the name MIS-C Associated with Coronavirus Disease 2019. The New York experience largely corroborates the European experience and adds that many of these children were resistant to intravenous immunoglobulin (IVIG), the typical treatment for Kawasaki disease, and needed steroids and sometimes immunomodulatory medication. Judicious fluid administration was also emphasized as many of these children have cardiovascular compromise. 6
Adolescent females can present with a wide spectrum of gynecologic complaints and the differential diagnosis can be broad. It is important for providers to be familiar with common gynecologic conditions and their treatment, and when it is appropriate to refer to or consult a gynecologic specialist or refer to the emergency room (ER). Below is an overview of some of the most common adolescent gynecologic diagnoses and management recommendations.
Abnormal Uterine Bleeding (AUB)
AUB is defined as menses outside the range of normal defined as: every 21-45 days, last < 7 days, and < 6 pads or tampons per day. Menses can be irregular for 2-3 years after menarche, however, no adolescent should go more than 3 months without a menses. The most common causes of irregular menses and/or prolonged heavy menses include anovulation due to endocrine causes or immaturity of the hypothalamic pituitary axis and bleeding disorders, the most common being Von Willebrand Disease. Work up for irregular menses includes TSH, Prolactin, LH, FSH, Estradiol, 17 OHP, testosterone, and gonorrhea/chlamydia if sexually active. A bleeding disorder work up is warranted if girls are consistently having prolonged heavy menses leading to anemia, flooding, doubling up pads, or other concerning symptoms such as easy bruising or gum bleeding. Recommended work up includes CBC, coagulation panel, TSH, and Von Willebrand Panel. Menses can be controlled with combined (estrogen/progesterone) hormonal contraceptives (pill, patch, ring) or progesterone only options (pill, injection, arm implant, and intrauterine device) which are ideally initiated after hormone work up for AUB is completed. Girls warrant referral to the ER if they have prolonged bleeding leading to significant anemia (hemoglobin < 8), soaking 1 pad or tampon per hour, or have symptomatic anemia. Heavy menstrual bleeding can be stopped acutely with the assistance of combined hormone pill taper or progesterone only pill taper (e.g. norethindrone acetate).
Abdominal and Pelvic Pain
The differential diagnosis for gynecologic causes of abdominal pain is broad including: dysmenorrhea, ovarian masses, pelvic inflammatory disease, and mullerian anomalies. Treatment for dysmenorrhea includes scheduled NSAIDS starting 1-2 days prior to menses and lasting throughout followed by hormonal contraception if treatment fails. Persistent abdominal pain not relieved by NSAIDS or acute severe pelvic pain warrants a pelvic ultrasound to evaluate the uterus and adnexa (ovaries/fallopian tubes). Adnexa > 5 cm with severe abdominal pain, nausea and vomiting warrant ER evaluation given the concern for ovarian torsion. Pelvic inflammatory disease is defined as uterine, adnexal, or cervical tenderness plus abdominal pain and should be prophylactically treated in any girl who is sexually active. Reasons for referral to the ER include nausea/vomiting, unable to tolerate oral medications, fever, or failed outpatient treatment. Obstructive mullerian anomalies such as imperforate hymen or non-communicating uterine remnants should also be considered when a patient has cyclical monthly pain or on examination has breast development and no vaginal opening. Patients with these diagnoses warrant ER evaluation if they have uncontrolled pain or difficulty with urination.
Vulvar Trauma and Genital Ulcers
Straddle injuries are very common and warrant ER evaluation when a large laceration is present, persistent bleeding, or large vulvar hematoma causing severe pain or inability to urinate. Most vulvar hematomas, though frightening on examination, will resolve with conservative management (NSAIDS, ice, rest) on their own. Lipshultz or aphthous vulvar ulcers should be in the differential for genital ulcers. It is a diagnosis of exclusion after diagnoses such as HSV. They are commonly caused by a viral illness (e.g. upper respiratory illness or gastroenteritis) and typically present 3-4 days after prodromal viral symptoms. Treatment is symptomatic including scheduled pain medication and topical or oral steroids. Indications for referral to the ER include uncontrolled pain and difficulties with urination.
Pediatric and Adolescent Gynecology in Atlanta!
Krista Childress, MD and Abigail Smith, PA-C are two pediatric gynecology providers at Children’s Healthcare of Atlanta that see patients birth to 21 years of age and treat a broad spectrum of gynecologic conditions from menstrual issues, contraceptive counseling, pre-pubertal complaints to surgical conditions including ovarian cysts and uterine/vaginal abnormalities. Don’t hesitate to reach out to Krista Childress, MD or Abigail Smith, PA-C for consultations, clinical questions, or patient referrals. They can be contacted at krista.childress@emory.edu or Abigail.smith@choa.org or Pediatric and Adolescent Gynecology Clinic at (404)-785-1491. Please see their website for information and referral links: https://www.choa.org/medical-services/gynecology.
When Karen Carpenter died of heart failure in 1983 from Anorexia nervosa, it raised awareness about the complications of eating disorders. Before her death there wasn’t much discussion about eating disorders and the dangers of rapid weight loss. Until recently, eating disorders were considered the most lethal of the mental health disorders. Now it is only second to opiate abuse as the most lethal of these conditions.
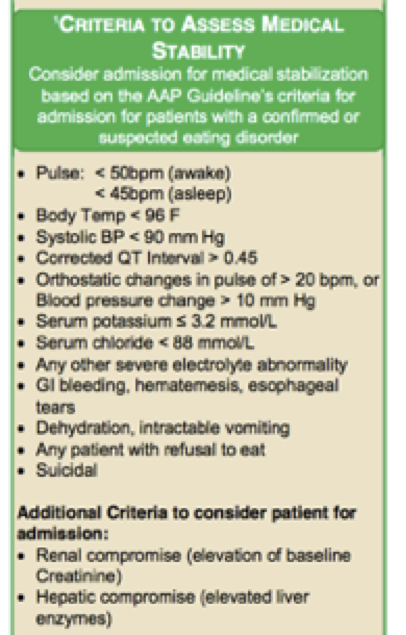
Eating Disorder Admissions at Children’s Healthcare of Atlanta Recently, we have seen an exponential increase in the admissions of patients with Eating Disorders at Children’s Healthcare of Atlanta. The incidence has increased exponentially from 18 admissions in 2010 to over 110 in 2018. Eating Disorders are mental illnesses that can have serious medical complications that can affect almost every organ system. The median age of onset is 12-13 years of age, and it can affect both genders. There has also been an increase in the diagnosis of eating disorders among the transgender population. At Children’s Healthcare of Atlanta, there are protocols in place for the management of these patients in the ED and inpatient services. This assists in early recognition and triage of these patients as they are evaluated to see if they warrant admission for medical stabilization (see chart end of article). The American Academy of Pediatrics has come up with a list of objective criteria to help with determining who warrants admission to the hospital. This includes such objective measures as vital signs (i.e. heart rates < 50 beats per minute), electrolyte criteria (such as phosphorus < 3.0), and consideration of patients that are most at risk of refeeding syndrome. It is the hope that this triage system will help with early recognition of patients with these disorders and help with admitting those who warrant medical stabilization.
Atypical Anorexia Nervosa Some of the most challenging patients to recognize are those with atypical Anorexia nervosa. By definition these patients would meet DSM-V criteria for the condition except that they may present with a normal weight and/or BMI. This can make it a challenge to recognized and this is why these patients may present later or more ill-appearing, given if they are looked at as a single plot on the growth chart they may look like their weight or BMI is within normal range. In conclusion, it is important to ask questions when a symptom raises a concern about an eating disorder. Is the patient overly concerned about his or her weight? Have they recently adopted a radical diet change, such as converting to a vegan diet? Have they developed primary or secondary amenorrhea? Or on their growth chart, have they plateaued or failed to achieve appropriate increases in their growth over time.? If you do have concerns about a patient that may have an eating disorder, it may be worth having them triaged at one of our Children’s Healthcare of Atlanta facilities. There if they meet criteria for medical stabilization, they can be admitted to our inpatient unit at Scottish Rite. We have a multidisciplinary team that includes psychiatry, hospitalist medicine, case management, nutrition and child life. Our goal is to help manage these patients medically and then transition them to an appropriate level of care post-discharge that could involve inpatient eating disorder treatment or outpatient therapy, depending on the needs of the patient and family. Contact information: Laura Doerr, MD, FAAP. Laura.doerr@choa.org
Ricardo Jimenez, Pediatric Emergency Medicine Physician
As physicians working in acute care centers or emergency departments, it’s a daily challenge dealing with patients who are intoxicated. But as new street drugs emerge in the community this challenge is even more difficult. Street drugs or designer drugs, are those drugs that are produced by “street pharmacists” at home or in clandestine laboratories. The goal of these drugs is to mimic the most common general classes of drugs that are abused. These new designer drugs are more easily found and affordable than their counterparts, most of them can be found on the internet or local smoke shops, and are considered “legal highs”. Because the street drug’s chemical composition is different from those that they try to mimic, in most cases the US DEA has no jurisdiction over them. At the same speed that the DEA is developing laws to govern these new chemicals, the street pharmacists can easily change the chemical composition, thus avoiding the DEA’s jurisdiction. To be prepared to manage intoxications from these new designer drugs, the physician must have a strong knowledge of the common drugs of abuse toxidromes. It’s impossible in the length of this article to discuss all the common designer drugs. I will discuss those that mimic the most common general classes of drugs of abuse; Synthetic Cannabinoids, Synthetic Cathinones and opioid analogues.
Lauren Middlebrooks, MD Pediatric Emergency Medicine Physician
Vaping-Related illness has plagued over 2,000 people this year alone, and has claimed the lives of now 47 innocent victims. Several deaths have been linked to the explosion of vape pen devices, however of greater concern is a “mysterious respiratory illness” that the CDC is now calling EVALI—e-cigarette or vaping-related lung injury.
Mike Greenwald, Pediatric Emergency Medicine Physician
CME 1.0 credit available complete after reading all 3 articles-Link at the end !
Those of us who practiced medicine in the previous century (“OK Boomer” – there, I said it) can tell our younger colleagues stories about the limitations we used to face in treating sick and injured children. We recall a time before we had eradicated some deadly diseases with vaccines, before we had pediatric specific approaches to trauma and many medical diseases and before we developed so many ready options for imaging and other studies. Yes, 2019 doctors struggle with different challenges. We all still work very hard. EMR has solved some problems and created others. Perhaps just as challenging – we are not quite as tight nit a medical community compared to when we were smaller. We rely on a growing number of often unfamiliar colleagues to help care for children in our community. That distance naturally leads to challenges and even barriers in communication and collaboration.
So this article is an attempt to share some issues from one side of a relationship. We asked faculty in our group to answer the question: “What do you wish referring primary care providers would better understand to improve the care we deliver to our patients?” Like any survey – this one has limitations. We recall negative experiences more vividly than positive ones. The truth is that the vast majority of referrals we get are clear, appropriate and helpful. What follows is a summary of observations of what might make a more effective transition of care. Perhaps none of these apply to you – but we hope that at least some of what you read here makes sense and you find useful. As always – we welcome your feedback and on-going collaboration with us so we can improve our role in helping care for your patients.
Be explicit in your concern. The families sent in to see us often assume that we have comprehensive knowledge of their medical issues. They may bring with them a brief note with vague information or simply neglect to tell us that you sent them in. Like a game of telephone the details can easily change.
What exactly is the purpose of this referral? If your concern is based on test results please share those details – especially growth chart data for the failure to thrive concern and lab or radiology results outside the CHOA system. Be clear in your call in whether you want a call back and provide the best contact number possible (ideally a direct #). If you haven’t heard from us please don’t hesitate to call the transfer center to speak with the treating physician. We may have every intention of calling you as requested but neglect to do so in the flurry of a busy shift.
Use the Transfer Center (404-785-7778). When you call in a patient you have the option to simply leave a message or to speak with one of us. Either way – your call in information is recorded in the chart and highlighted by the patient’s name with a letter “C” next to their name. This reminder is intended to guide us to your note.
We understand that you are busy and sometimes it takes more time than we’d like to speak with someone in the transfer center. Like the ED volumes – the transfer center calls can vary dramatically. In fact – the CHOA Transfer Center is the busiest Pediatric Hospital Transfer Center in the Country! It is staffed with 1-5 nurses at a time 24/7 based on volume patterns – with plans to increase staffing with our up coming move at the North Druid Hills campus. In addition, they are actively working on new ways to streamline the process.
We want to speak with you! We often get patients with a concern that could have been addressed with a conversation on the phone with either an ED doc or other sub specialist. Some of the patients could have been a direct admission; others would eventually be sent to a specialty clinic. Not sure if ED referral is the best option for this patient? Call us! The Transfer Center can facilitate this – typically in less than 15 minutes.
Please understand when you are waiting to speak with us the Transfer Center nurse is diligently requesting us to answer the call. Your wait is only because we a caring for patients; but when we are at a desk charting we will stop and pick up the phone. We would much rather spend 5 minutes chatting with you about your concerns rather than explain to your patient why we can’t do what was expected when they finally get into a room after a long wait.
Sign out patient info to your on call colleague. It seems to be a common occurrence that when we call a practice after hours the on call doc knows nothing about the patient sent in by their colleague. That can make our evaluation more challenging than necessary. A brief sign out can go a long way to ensure accurate communication and effective follow-up.
Be clear and careful regarding expectations. You might be surprised at how often we get a family who says they were told they would see a subspecialist in the ED or get a specific study performed. (Yes, we know that they may have distorted what you told them). We don’t dispense nebulizers and seldom can get an MRI. While we can speak by phone with our subspecialty colleagues, it is simply not feasible (nor necessary) for them to see each patient presenting in the ED. Also, we try to follow guidelines to reduce unnecessary testing so head injured patients may be assessed clinically without imaging and children with flu-like illnesses may be diagnosed clinically rather than with a flu test.
If you have an urgent question for a specific sub specialist consider using the transfer center to speak with them. Contact radiology if you want to expedite or ask about a specific imaging study. Like the surgeon who evaluates abdominal pain or the cardiologist who assesses a murmur, the ED physician will choose tests and treatments for patients based on their training and experience.
Be judicious about sending in contagious or vulnerable patients such as neonates. This is particularly important this time of year when the waiting room may be filled with children experiencing influenza. Each year it seems we get a surge of flu positive patients who were recently seen in our ED for an unrelated problem. They may have presented without the flu but left with it! Also in that waiting room are neonates and immuno-compromised children. If you are concerned about a dangerous infection such as TB or Measles – lets talk before sending in the patient!
CLICK on Link below to receive CME Credit after reading all 3 articles!!!!
By Jennifer Plagemann, Paramedic; Ryan Sullivan, RN; Simeon Smith, Paramedic; and Rebecca Ogrin, RN
The Children’s Healthcare of Atlanta transport team is excited to spread the word about our Transport Program. As a direct extension of the Children’s Emergency Departments and Intensive Care Units, we pride ourselves on providing the highest level of pediatric care. We look forward to introducing our team and explaining some of the capabilities that separate us from other transport options.
Transport requests begin in our Communications Center, where communications specialists are advanced EMTs and paramedics with specialized training in triage and pediatric critical care. They work in collaboration with the Children’s Transfer Center to expedite dispatch times and facilitate appropriate modes of transport. Our communications specialists also keep our teams connected to Children’s emergency physicians and intensivists for real-time consultations and care recommendations.











{kind=link}