Viral bronchiolitis is a leading cause of hospitalization in the first year of life. While supportive care is the mainstay of bronchiolitis management, the medical community continuously searches for treatments to improve patient outcomes. Unfortunately, rigorous studies often fail to detect widespread benefit of these previously promising therapies (e.g., albuterol, steroids).1 The use of one such hopeful therapy, heated and humidified high flow nasal cannula (HFNC), has increased dramatically over the last 10 years both in the ICU and general care area. However, in the same time frame, bronchiolitis admissions have decreased while medical costs and ICU utilization have increased (correlation, not causation!).2-6
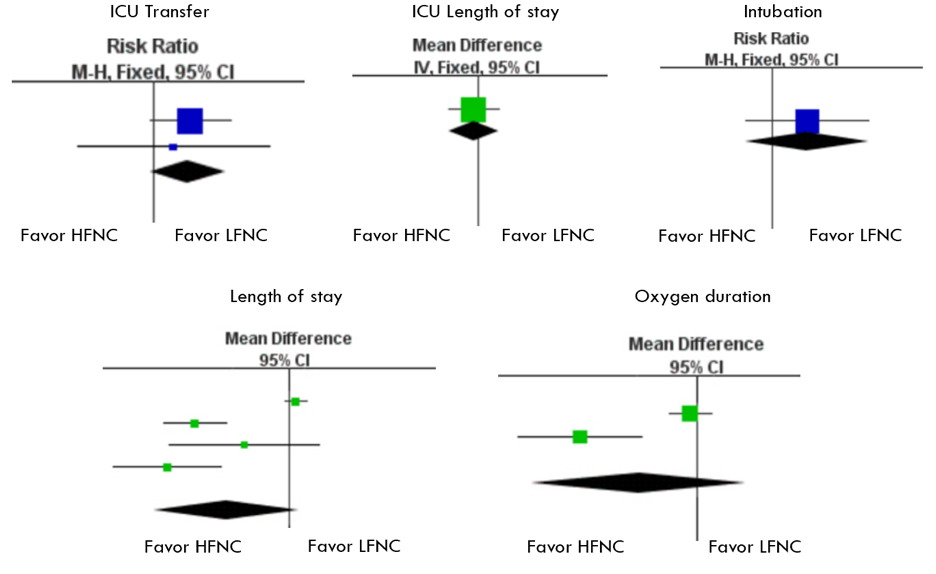
There are now three randomized controlled trials (RCTs) to help evaluate whether HFNC improves bronchiolitis care.7-9The RCTs, which included 1942 patients with moderate bronchiolitis, compared clinical outcomes between patients randomized to early treatment with HFNC to those randomized to early low-flow nasal cannula (LFNC). These studies and a meta-analysis found no difference in clinically meaningful outcomes between early versus late (aka rescue) use of HFNC therapy – including length of stay, ICU utilization, and intubation rates, which were low. The below forest plots from the meta-analysis visually demonstrate this – the bottom diamond crosses the centerline for all measures, indicating no significant difference between early LFNC and early HFNC.10